
BRCA mutations drive a biologically distinct and aggressive form of mCSPC1
PROGNOSIS
Patients with BRCAm mCSPC often face considerably worse prognoses than those without this mutation1
 Faster disease progression
Faster disease progression Reduction in survival
Reduction in survivalPrevious standard of care (SoC) treatment approaches have often been inadequate in these patients1
GUIDELINES
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for mCSPC recommend testing for mutations before systemic treatment2
- The panel strongly recommends a metastatic biopsy for histologic and molecular evaluation. When unsafe or unfeasible, plasma ctDNA assay is an option, preferably collected during PSA and/or radiographic progression in order to maximize diagnostic yield
- Patients should be informed that tumor testing may uncover germline findings, and confirmatory germline testing may be recommended to inform familial risk
Testing
Test for and target BRCAm to optimize patient care
Multiple, accessible options are available for robust genetic testing, including2-4:
Tissue or liquid biopsy
For initial prognostic testing using next-generation sequencing
Tumor testing for somatic alterations
At first metastases or signs of progression
Your patients with mCSPC may benefit from getting retested for BRCA m, as tumor mutations can accumulate over time.4
Precision Medicine
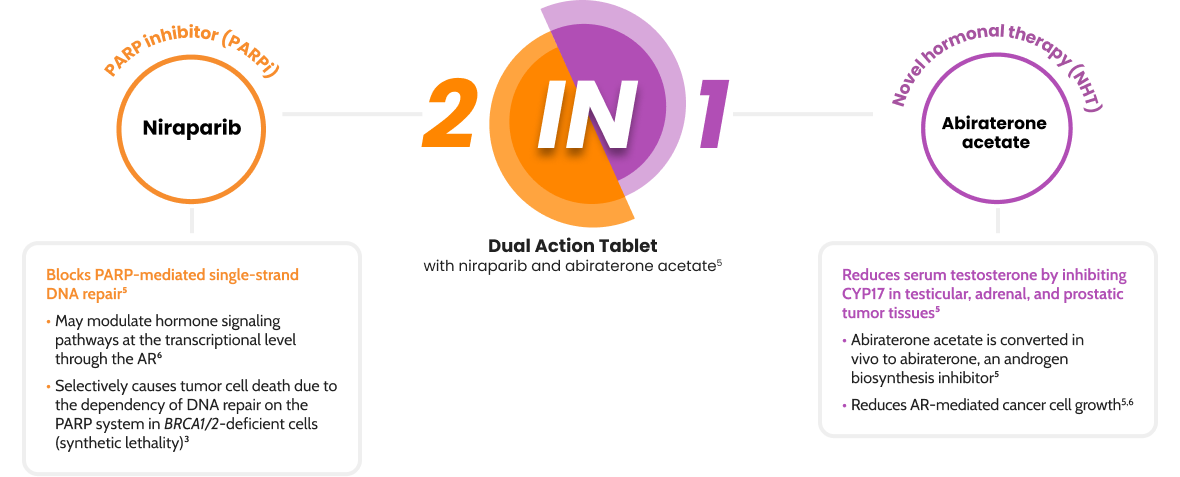
AKEEGA® is the first FDA-approved targeted therapy in BRCA2 m mCSPC5
Only AKEEGA® combines the precision of PARP inhibition with an NHT into a dual action tablet5

Test early, then target BRCA2 m with AKEEGA®
References:
- Olmos D, Lorente D, Jambrina A, et al. BRCA1/2 and homologous recombination repair alterations in high- and low-volume metastatic hormone-sensitive prostate cancer: prevalence and impact on outcomes. Ann Oncol. 2025;36(10):1190-1202.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Prostate Cancer V.4.2026. © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed December 18, 2025. To view the most recent and complete version of the guideline, go to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
- Teyssonneau D, Margot H, Cabart M, et al. Prostate cancer and PARP inhibitors: progress and challenges. J Hematol Oncol. 2021;14(1):51.
- Cheng HH, Sokoloba AO, Schaeffer EM, et al. Germline and somatic mutations in prostate cancer for the clinician. J Natl Compr Canc Netw. 2019;17(5):515-521.
- AKEEGA® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
- Schiewer MJ, Goodwin JF, Han S, et al. Dual roles of PARP-1 promote cancer growth and progression. Cancer Discov. 2012;2(12):1134-1149.